TABLE OF CONTENTS
- Introduction
- Facts that Shaped the Dispute
- Proceedings Before Consumer Fora
- Core Questions Before the National Consumer Disputes Redressal Commission
- Substantive Justice Over Procedural Technicality
- Statutory Framework Governing Medical Practice
- Supreme Court Jurisprudence and Unauthorized Medical Practice
- Unauthorized Prescription as Negligence Per Se
- Access to Justice and the Institutional Role of Legal Aid
- Expert Perspective: Implications for Medical Regulation and Consumer Jurisprudence
- Relief Granted by the Commission
- Conclusion
- Frequently Asked Questions (FAQs)
Introduction
The jurisprudence governing medical negligence in India has progressively evolved through the intersection of professional accountability and consumer protection law, transforming patient rights from abstract expectations into enforceable statutory entitlements. Judicial recognition of medical services as falling within the ambit of “service” under consumer legislation has significantly expanded access to remedies, enabling individuals to challenge deficient or unlawful treatment before specialized adjudicatory fora designed to deliver expeditious and affordable justice. Consumer fora, therefore, no longer function merely as compensatory mechanisms but as institutional safeguards ensuring regulatory discipline within service-based professions affecting public health and safety.
Within this broader framework, the statutory regulation of modern medicine assumes critical importance. Unauthorized medical intervention is not confined to questions of professional ethics alone; it implicates patient safety, public confidence in healthcare delivery, and the uniform enforcement of national medical standards. In semi-urban and rural healthcare markets, where optical centres and allied practitioners frequently operate at the intersection of diagnostic assistance and clinical treatment, the blurring of professional boundaries exposes vulnerable patients to substantial risk arising from unqualified medical decision-making.
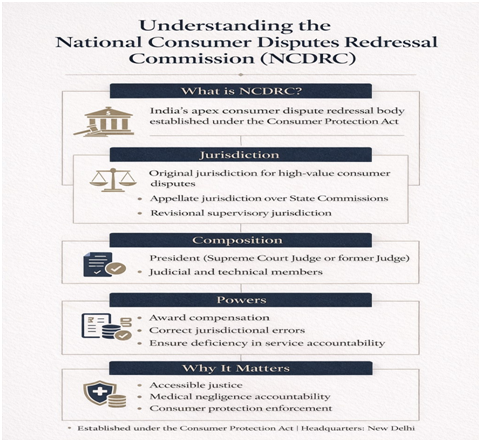
Against this backdrop, the National Consumer Disputes Redressal Commission (NCDRC), New Delhi, in Rakesh Kumar Shukla v. Alok Eye Health and Optical Centre (Revision Petition No. NC/RP/574/2025, decided on 30 January 2026), delivered a significant reaffirmation of statutory discipline in medical practice. The Commission held that prescription of allopathic medicines by a person lacking recognized medical qualification and statutory registration constitutes negligence by operation of law and amounts to a clear deficiency in service under consumer protection jurisprudence. The ruling arose from a dispute involving permanent loss of vision allegedly caused following treatment administered at an optical establishment, where handwritten prescriptions and administration of medicines by an unqualified individual formed the core controversy.
Beyond resolving the individual grievance, the judgment underscores the supervisory role of consumer fora in correcting jurisdictional errors committed by subordinate bodies and reinforces the constitutional objective of access to justice. Equally significant is the intervention of the Delhi State Legal Services Authority (DSLSA), illustrating how structured Legal Aid representation can enable economically constrained litigants to pursue complex medico-legal disputes through successive adjudicatory stages and ultimately secure substantive justice.
Facts that Shaped the Dispute
The dispute emerged from a sequence of events commencing on 9 June 2010, when the complainant experienced redness and discomfort in his left eye. On the following day, 10 June 2010, he approached the respondent’s optical establishment seeking treatment. According to the record, the respondent examined the affected eye, administered oral medicines and eye drops, and prepared a handwritten prescription containing allopathic drugs while receiving ₹500 in cash towards consultation and treatment charges. The absence of a formal receipt subsequently became central to the controversy regarding maintainability before the consumer fora; however, affidavit evidence later substantiated payment of consideration.
Soon after the treatment, the complainant’s condition deteriorated progressively. The left eye developed a severe infection accompanied by increasing pain and functional impairment. On 11 June 2010, the complainant travelled to Bahraich and consulted ophthalmologist Dr. A.K. Mishra, who diagnosed that the infection had developed following administration of the medicines prescribed by the respondent. Seeking further medical evaluation, the complainant consulted another specialist, Dr. Kishan Lal, on 19 June 2010, who confirmed that the eye had become completely infected.
Despite these consultations, the infection remained uncontrolled. Consequently, on 10 July 2010, the complainant was admitted to the Dr. Rajendra Prasad Centre for Ophthalmic Sciences, New Delhi, for advanced treatment. Notwithstanding sustained medical intervention at a specialised tertiary care institution, the infection proved irreversible, resulting in permanent loss of vision in the left eye.
The complainant incurred medical expenditure approximating ₹2,00,000 during the course of treatment, apart from enduring permanent physical impairment affecting daily functioning and livelihood. Aggrieved by the alleged negligent and unauthorized medical intervention, he instituted a consumer complaint under Section 12 of the Consumer Protection Act, 1986 seeking compensation for medical negligence and deficiency in service.
Proceedings Before Consumer Fora
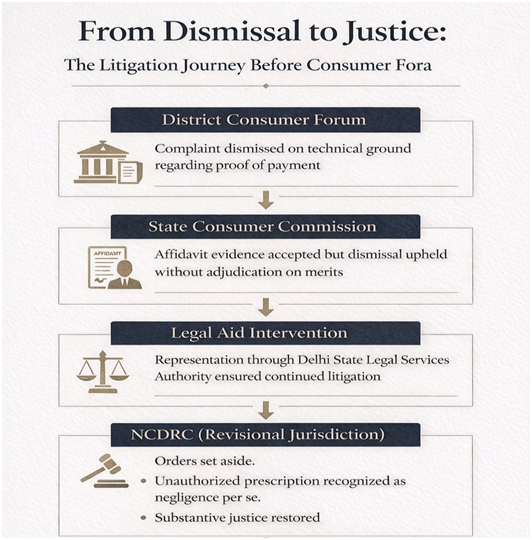
The procedural history of the dispute demonstrates how technical interpretation of statutory requirements may obstruct substantive adjudication when consumer jurisdiction is narrowly exercised. The District Consumer Disputes Redressal Forum dismissed the complaint principally on the ground that payment of consultation charges had not been sufficiently proved. Holding that absence of documentary proof disentitled the complainant from qualifying as a “consumer” under Section 2(1)(d) of the Consumer Protection Act, 1986, the Forum declined to examine the substantive allegations relating to unauthorized prescription, medical negligence, causation, and loss of vision.
This approach effectively terminated the proceedings at the threshold stage without adjudicating determinative issues arising from the pleadings and evidence. The State Consumer Commission, in appeal, accepted affidavit evidence regarding payment of ₹500 as consultation charges and thereby acknowledged the existence of a consumer–service provider relationship. However, instead of remanding the matter for adjudication on merits, it upheld dismissal and proceeded to record findings suggesting that a diploma holder could prescribe allopathic medicines.
The failure to restore adjudication after recognizing maintainability created a clear jurisdictional inconsistency. Aggrieved by concurrent dismissal and alleged misapplication of statutory law, the complainant invoked the revisional jurisdiction of the National Consumer Disputes Redressal Commission seeking corrective intervention.
Core Questions Before the NCDRC
In exercise of its revisional jurisdiction, the National Consumer Disputes Redressal Commission was required to address questions extending beyond a routine factual dispute and touching upon the proper discharge of statutory adjudicatory responsibility by consumer fora. The determinative issues before the Commission were:
- Whether dismissal of the complaint solely on the ground of maintainability amounted to abdication of jurisdiction when substantive allegations of negligence required adjudication.
- Whether a diploma holder in optometry or an allied field possessed statutory authority under governing central legislation to prescribe allopathic medicines.
- Whether prescription of modern medicine by an unqualified and unregistered individual constitutes negligence per se and a deficiency in service under consumer protection law.
These questions engaged both regulatory compliance and institutional accountability within consumer adjudication.
Substantive Justice Over Procedural Technicality
The NCDRC delivered a strong institutional critique of the approach adopted by the fora below, holding that procedural formalism cannot override the statutory obligation to adjudicate substantive disputes arising under consumer legislation. The District Forum dismissed the complaint solely on the preliminary ground that payment of consultation charges had not been conclusively proved and, consequently, declined to examine allegations concerning unauthorized prescription, negligence, causation, and permanent injury. The Commission observed that such disposal amounted to an abdication of jurisdiction, as consumer fora are statutorily mandated to determine disputes relating to deficiency in service once material indicating provision of treatment and consideration exists.
Equally significant was the error committed by the State Commission. Having accepted affidavit evidence as sufficient proof of payment and thereby recognizing the complainant as a consumer, it ought to have remanded the matter for adjudication on merits, particularly when no findings had been returned on determinative issues. Instead, the appellate forum proceeded to affirm dismissal while recording legally unsustainable observations regarding the respondent’s authority to prescribe medicines.
The decision reinforces an established judicial principle that consumer adjudication must prioritize substantive justice over hyper-technical procedural barriers, particularly where allegations involve serious bodily injury and denial of effective medical care.
Statutory Framework Governing Medical Practice
Central to the controversy was the statutory legality of prescribing modern (allopathic) medicine. The regulatory framework governing medical education, professional qualifications, and standards is substantially occupied by Parliamentary legislation, namely the Indian Medical Council Act, 1956, now succeeded by the National Medical Commission Act, 2019. Section 15(1) and Section 15(2) of the 1956 Act expressly prohibit any person from practising modern medicine or prescribing allopathic drugs unless such individual possesses a recognised medical qualification included in the statutory schedules and is duly registered in the State Medical Register.
The constitutional foundation of this regulatory scheme lies in Entry 66 of List I (Union List) of the Seventh Schedule, which vests Parliament with authority over coordination and determination of standards in higher education and professional practice. Consequently, State-level recognitions, diplomas in optometry, or allied professional qualifications cannot dilute or override central statutory restrictions governing medical practice.
The NCDRC reaffirmed that uniform national standards in healthcare regulation must prevail over fragmented local authorisations, ensuring that prescription of modern medicine remains confined to duly qualified and registered practitioners.
Supreme Court Jurisprudence and Unauthorized Practice
The NCDRC anchored its determination within a well-settled line of Supreme Court jurisprudence governing professional accountability in medical practice and consumer protection law. Reliance was placed upon Baharul Islam & Ors. v. Indian Medical Association & Ors., wherein the Supreme Court clarified that regulation of medical education and standards is substantially occupied by central legislation, and that diploma holders or rural practitioners cannot claim authority to prescribe allopathic medicines in derogation of statutory mandates.
The doctrinal foundation of consumer oversight over medical services traces back to Indian Medical Association v. V.P. Shantha, which recognized healthcare as a “service” within the meaning of consumer legislation, thereby enabling patients to seek remedies for deficient professional conduct before consumer fora.
Equally significant was Poonam Verma v. Ashwin Patel, where the Court held that practising a system of medicine without requisite qualification constitutes negligence per se, dispensing with the need for further inquiry into professional competence. Complementing this principle, Jacob Mathew v. State of Punjab emphasized adherence to reasonable standards of professional skill and care as the touchstone of medical liability.
Synthesizing these authorities, the NCDRC reaffirmed that violation of statutory qualification requirements itself may establish negligence and consequent deficiency in service.
Unauthorized Prescription as Negligence Per Se
One of the most significant doctrinal contributions of the decision lies in the Commission’s recognition of unauthorized prescription as negligence by operation of law. The NCDRC held that where central legislation expressly restricts the practice and prescription of modern medicine to duly qualified and registered practitioners, any deviation from such statutory mandate constitutes deficiency in service independent of further evidentiary inquiry. The requirement of professional competence or intention becomes secondary once the foundational illegality of practice is established.
Relying upon the statutory prohibition contained in Section 15 of the Indian Medical Council Act, 1956, as interpreted in binding Supreme Court precedent, the Commission clarified that a diploma in optometry or any allied qualification does not confer authority to prescribe allopathic medicines. Consequently, the very act of issuing a prescription by an unregistered and unqualified individual attracts legal liability irrespective of whether harm was intended or whether the treatment initially appeared beneficial.
By treating unauthorized prescription as negligence per se, the ruling significantly strengthens consumer protection within healthcare delivery. The approach is particularly relevant in semi-urban and rural settings where informal practitioners frequently blur professional boundaries, thereby exposing patients to irreversible medical risk and undermining statutory regulatory safeguards.
Access to Justice and the Institutional Role of Legal Aid
The proceedings also highlight the institutional significance of Legal Aid within consumer adjudication. Medical negligence litigation frequently demands sustained financial resources, procedural awareness, and technical legal expertise, factors that often discourage economically vulnerable litigants from pursuing remedies beyond initial adverse findings. In the present case, representation facilitated through the Delhi State Legal Services Authority (DSLSA) enabled the complainant to challenge concurrent dismissal orders and pursue revisional scrutiny before the National Commission.
Legal Services Authorities established under the Legal Services Authorities Act, 1987 are designed not merely to provide formal representation but to reduce structural barriers affecting meaningful access to justice. The matter exemplifies how institutional legal assistance can transform procedural setbacks into substantive adjudication by ensuring continued participation within the legal process. By enabling effective presentation of statutory arguments concerning unauthorized medical practice and consumer rights, Legal Aid support ensured that regulatory violations resulting in serious personal injury received judicial examination on merits rather than being foreclosed at preliminary stages.
Expert Perspective: Implications for Medical Regulation and Consumer Jurisprudence
According to Adv. Devendra Sabadra, the ruling reinforces statutory discipline in healthcare by affirming that professional convenience cannot dilute central regulatory mandates governing modern medical practice. The decision signals heightened medico-legal accountability, clarifying that unauthorized prescription itself attracts liability, while simultaneously strengthening consumer confidence in accessible adjudicatory mechanisms addressing regulatory violations affecting patient safety.
Relief Granted by the Commission
Allowing the revision petition, the National Consumer Disputes Redressal Commission set aside the concurrent orders of the District Forum and the State Commission, observing that the complaint had been dismissed without adjudication of the determinative issues relating to unauthorized medical prescription and resulting harm. Exercising its revisional jurisdiction, the Commission proceeded to grant substantive relief commensurate with the gravity of injury suffered by the complainant, whose permanent loss of vision was linked to treatment administered by a person lacking statutory authority to prescribe allopathic medicines.
The respondent was directed to pay compensation of ₹2,00,000 together with simple interest at 9% per annum from the date of institution of the complaint until realization, along with litigation costs of ₹20,000. The award underscores the remedial mandate of consumer fora, affirming that statutory violations affecting patient safety warrant meaningful compensatory intervention.
Conclusion
The decision marks a principled reaffirmation that statutory regulation of medical practice operates as a safeguard for public health rather than a mere professional formality. By correcting jurisdictional errors committed by the fora below and recognizing unauthorized prescription itself as actionable deficiency in service, the National Consumer Disputes Redressal Commission restored both doctrinal clarity and consumer confidence within healthcare litigation.
The ruling underscores that regulatory compliance is inseparable from patient safety, and that professional boundaries defined under central legislation cannot be diluted by convenience or local practice. Equally significant is the access-to-justice dimension of the case. Institutional legal aid enabled sustained representation despite successive adverse findings, demonstrating how structured advocacy can translate statutory rights into meaningful remedies.
Ultimately, the judgment sends an unambiguous message: unauthorized medical intervention attracts legal accountability, and consumer fora remain vital guardians against regulatory violations causing serious personal harm.
Frequently Asked Questions (FAQs)
Q1. Can diploma holders prescribe allopathic medicines?
No. Prescription of modern medicine requires a recognised medical qualification and registration under central legislation. Diplomas in optometry or allied fields do not confer such authority.
Q2. Does absence of a receipt defeat consumer status?
Not necessarily. Credible affidavit evidence and surrounding circumstances may establish payment and a consumer relationship.
Q3. What is negligence per se in medical law?
Negligence per se arises when conduct violates a statutory prohibition. Unauthorized prescription itself constitutes deficiency in service irrespective of intent.
Q4. Are medical services covered under consumer protection law?
Yes. Medical treatment falls within “service” where consideration exists, enabling patients to seek remedies before consumer fora.
Q5. Can consumer fora award compensation for medical negligence?
Yes. Consumer fora may grant compensation, interest, and litigation costs where statutory violation and resulting injury are established.
Q6. Why was Legal Aid representation significant in this case?
DSLSA assistance ensured continued advocacy after adverse findings, ultimately securing corrective supervisory intervention by the NCDRC.
Join LAWyersClubIndia's network for daily News Updates, Judgment Summaries, Articles, Forum Threads, Online Law Courses, and MUCH MORE!!"
Tags :Others